Online Therapy,
Matched by a Human.
Not a Quiz.
Other platforms assign you a therapist in 60 seconds. We take the time to actually understand what you need. Most clients are matched within 48 hours.



10,000+ clients helped · 4.8 ★ on the App Store

We accept many
insurance plans







Getting Started is Easy
Three simple steps to begin your mental health journey — no guesswork, no long waits.
Answer a Few Questions
Sign up in three minutes or less. Tell us what you're looking for and we'll handle the rest — or call a Care Coordinator directly.

Meet Your Therapist
Browse therapists matched to your needs, or let a Care Coordinator recommend the right fit for you.
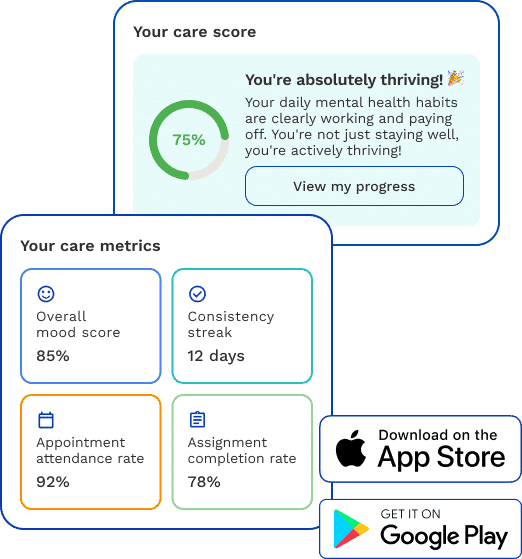
Measure Your Progress
Track your growth with personalized tools and regular check-ins. Your therapist adjusts your plan as you improve.

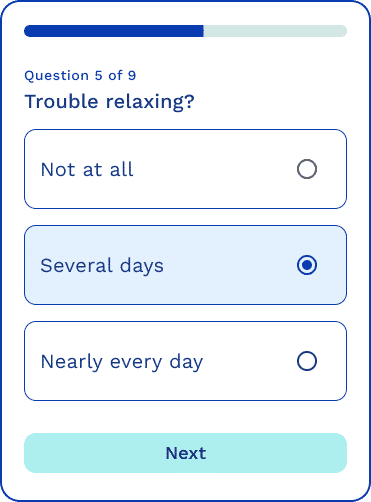
Take a Free, Quick
Mental Health Assessment.
Will therapy help? Find out with our confidential assessment — you'll understand potential challenges and receive personalized recommendations for support.
What Our Clients Are Saying
“ReachLink made it so easy to find a therapist who truly understood my needs. I was matched within 48 hours and started feeling better after just a few sessions.”
Sarah M.
Verified Customer · Google
“The care coordination team is outstanding. They walked me through everything and made sure I was comfortable before my first appointment. Highly recommend.”
James T.
Verified Customer · Google
“I was skeptical about online therapy but ReachLink changed my mind completely. My therapist is knowledgeable, compassionate, and always available when I need support.”
Maria L.
Verified Customer · Google
“Finally a platform that accepts my insurance! The app makes it easy to track my progress and I've noticed real improvements in just two months.”
David K.
Verified Customer · Google
“The matching process was spot-on. My therapist specializes exactly in what I needed help with. The sessions are convenient and the platform is easy to use.”
Aisha P.
Verified Customer · Google
“Getting started was so much easier than I expected. Within days I had my first appointment and felt heard for the first time in years. Thank you ReachLink.”
Carlos R.
Verified Customer · Google
As seen in




Get Real Support.
See Real Results.
Join thousands who have found the right therapist through ReachLink. Start today!
A care coordinator personally connects you with the right therapist, often within 48 hours.
No referral needed · Most insurance accepted · Start within 48 hours








